
 17 February, 2026
17 February, 2026
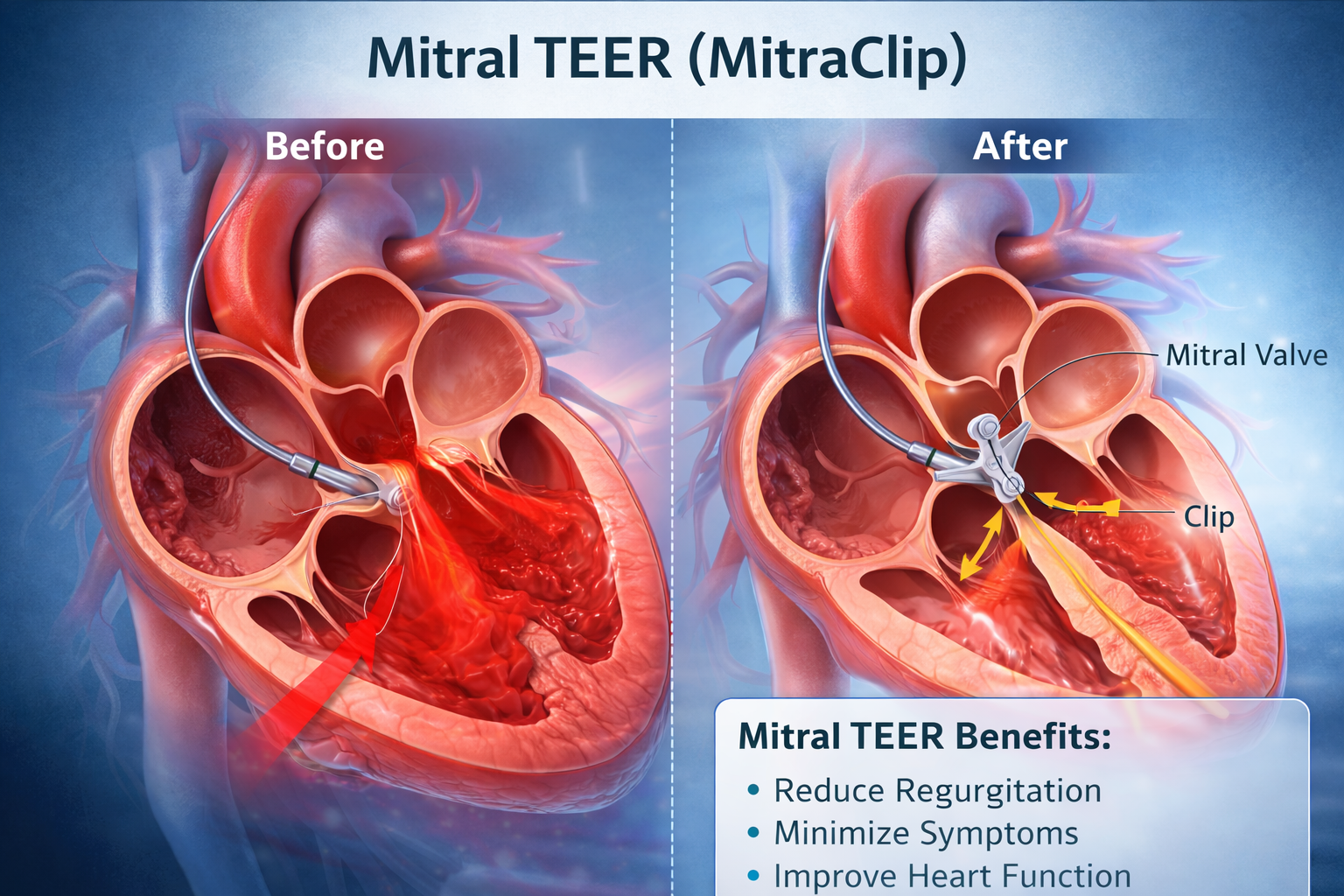
Mitral TEER (MitraClip) — Patient Selection is Everything
Mitral regurgitation (MR) is one of the most common valvular heart diseases worldwide. For decades, surgery was the only definitive solution. However, not all patients are ideal surgical candidates — especially elderly individuals, those with heart failure, or patients with multiple comorbidities.
This is where Mitral TEER (Transcatheter Edge-to-Edge Repair) has transformed modern cardiology.
Commonly performed using the MitraClip, Mitral TEER offers a minimally invasive alternative to open-heart surgery. But here’s the critical truth:
The success of Mitral TEER depends far more on patient selection than on the procedure itself.
Let’s explore why.
Understanding Mitral Regurgitation (MR)
The mitral valve sits between the left atrium and left ventricle. When it fails to close properly, blood leaks backward — a condition known as mitral regurgitation.
Over time, MR can lead to:
-
Breathlessness
-
Fatigue
-
Swelling in legs
-
Recurrent hospitalizations
-
Worsening heart failure
-
Reduced life expectancy
MR is broadly classified into:
1️⃣ Primary (Degenerative) MR
Caused by structural valve problems — leaflet prolapse, flail leaflet, chordal rupture.
2️⃣ Secondary (Functional) MR
Caused by left ventricular dysfunction — common in cardiomyopathy and heart failure.
The distinction matters tremendously when selecting TEER candidates.
What is Mitral TEER?
Transcatheter Edge-to-Edge Repair (TEER) is a catheter-based technique performed via the femoral vein. A device is guided into the heart and clips the anterior and posterior mitral leaflets together, reducing regurgitation by creating a double-orifice valve.
Unlike surgery:
-
No chest opening
-
No cardiopulmonary bypass
-
Faster recovery
-
Shorter hospital stay
But TEER is not for everyone.
Why “Patient Selection is Everything”
Mitral TEER is not a shortcut. It is not a universal replacement for surgery. Its success depends on selecting:
-
The right patient
-
At the right stage
-
With the right valve anatomy
-
And realistic expectations
Poor selection leads to:
-
Residual MR
-
Procedural failure
-
Early recurrence
-
No clinical benefit
Let’s break down what determines ideal candidacy.
1️⃣ Severity of Mitral Regurgitation
Only moderate-to-severe or severe MR qualifies.
Mild MR does not justify intervention.
Quantitative echo parameters typically evaluated:
-
Effective Regurgitant Orifice Area (EROA)
-
Regurgitant volume
-
Vena contracta width
Accurate echocardiographic assessment is critical.
2️⃣ Symptoms and Clinical Status
Mitral TEER is considered when patients have:
-
Persistent breathlessness
-
Recurrent heart failure admissions
-
Reduced quality of life
-
Symptoms despite optimal medical therapy
If the patient is asymptomatic, careful observation may be more appropriate.
3️⃣ Surgical Risk Assessment
TEER was initially developed for patients who are:
-
High surgical risk
-
Elderly
-
Frail
-
Having multiple comorbidities
-
Previous cardiac surgery patients
If surgical risk is low and anatomy favorable, surgery may still provide better long-term durability.
A multidisciplinary Heart Team decision is mandatory.
4️⃣ Valve Anatomy — The Deciding Factor
This is the most important element.
Ideal mitral valve anatomy for TEER includes:
-
Central jet (A2–P2 region)
-
Adequate leaflet length
-
Limited calcification
-
No severe leaflet restriction
-
Mitral valve area sufficient to avoid stenosis
Poor anatomy = poor outcomes.
Advanced imaging such as:
-
3D Transesophageal Echocardiography (TEE)
-
CT imaging
is essential before decision-making.
5️⃣ Primary vs Secondary MR — A Critical Difference
Primary MR
TEER works well in high-risk patients with degenerative MR when surgery is not feasible.
Secondary MR
In functional MR, patient selection must be extremely careful.
The landmark COAPT Trial showed:
-
Reduced hospitalizations
-
Improved survival
-
Significant symptomatic relief
But another study, MITRA-FR Trial, showed no significant benefit.
Why the difference?
Because patient selection varied. The proportion of MR relative to LV dysfunction matters.
This concept is often referred to as:
Disproportionate vs Proportionate MR
Only selected secondary MR patients benefit significantly.
6️⃣ Left Ventricular Function
If the ventricle is too dilated or severely dysfunctional, reducing MR may not reverse heart failure.
TEER works best when:
-
LV is not extremely dilated
-
MR is a major contributor to symptoms
Timing matters.
Too early — unnecessary.
Too late — ineffective.
Benefits of Properly Selected Mitral TEER Patients
When done in the right patient:
-
Immediate reduction in MR
-
Improved exercise tolerance
-
Reduced hospital admissions
-
Improved survival (selected cases)
-
Better quality of life
Recovery is usually rapid — many patients discharged within 48–72 hours.
Risks and Limitations
Though minimally invasive, TEER is not risk-free.
Possible complications:
-
Vascular injury
-
Residual MR
-
Mitral stenosis
-
Device detachment
-
Need for future surgery
However, in experienced centers, complication rates are low.
The Role of the Heart Team
Mitral TEER should never be a single-physician decision.
The Heart Team includes:
-
Interventional cardiologist
-
Cardiac surgeon
-
Heart failure specialist
-
Imaging cardiologist
-
Anesthesiologist
Comprehensive evaluation ensures:
-
Right indication
-
Right timing
-
Right strategy
The Future of Mitral TEER
Technology continues to evolve:
-
Next-generation clip systems
-
Wider grasping range
-
Improved leaflet capture
-
Combination therapies
-
Transcatheter mitral valve replacement (TMVR) development
But even with advanced devices, patient selection will remain the cornerstone.
Key Takeaways
Mitral TEER is revolutionary.
But it is not a blanket solution.
Success depends on:
✔ Severe MR
✔ Persistent symptoms
✔ Optimized medical therapy
✔ Favorable valve anatomy
✔ Appropriate surgical risk
✔ Multidisciplinary decision-making
In structural heart interventions, judgment matters more than technology.
And in Mitral TEER —
Patient Selection is Everything.
Frequently Asked Questions (FAQs)
1. Is MitraClip the same as open-heart surgery?
No. MitraClip is a catheter-based procedure performed through a vein without opening the chest.
2. How long does the MitraClip procedure take?
Typically 1.5–3 hours, depending on complexity.
3. Is general anesthesia required?
Most cases are performed under general anesthesia to allow precise imaging guidance.
4. How long is hospital stay?
Usually 2–3 days if there are no complications.
5. Is the clip permanent?
Yes. The device remains permanently attached to the valve.
6. Can MR return after TEER?
Yes, especially if anatomy was borderline or disease progresses.
7. Is TEER suitable for young patients?
Surgery is usually preferred in young, low-risk patients with degenerative MR due to durability.
8. Does TEER cure heart failure?
It reduces MR-related burden but does not cure underlying cardiomyopathy.
9. What tests are needed before the procedure?
-
Echocardiography (TTE & TEE)
-
CT scan (selected cases)
-
Coronary angiography
-
Blood investigations
10. Who should I consult for Mitral TEER?
A structural heart specialist or interventional cardiologist in a center offering advanced valve therapies.
Dr. A. B. Gopalamurugan
MD, MRCP, FRCP, CCDS, FACC
Dr. A. B. Gopalamurugan is a London-based Cardiologist with over 20 years of experience.
He is a renowned pioneer in:
-
Interventional Cardiology
-
TAVR (Transcatheter Aortic Valve Replacement)
-
Electrophysiology
-
Endovascular Aortic Repairs
Consultation Locations
🇬🇧 London
W1 Healthcare
7 Russell Gardens,
London W14 8EZ,
United Kingdom
📞 +44 7425 861747
🇮🇳 Chennai
2nd Floor, 46 & 48, Masilamani Rd,
Balaji Nagar, Royapettah,
Chennai, Tamil Nadu 600014
📞 080560 88898
🇮🇳 Mumbai
81–84, Indian Cancer Society
Formerly Lady Ratan Tata Medical & Research Centre
M. Karve Road, Cooperage St,
Mumbai, Maharashtra 400021
📞 089400 88898



