
 22 April, 2026
22 April, 2026
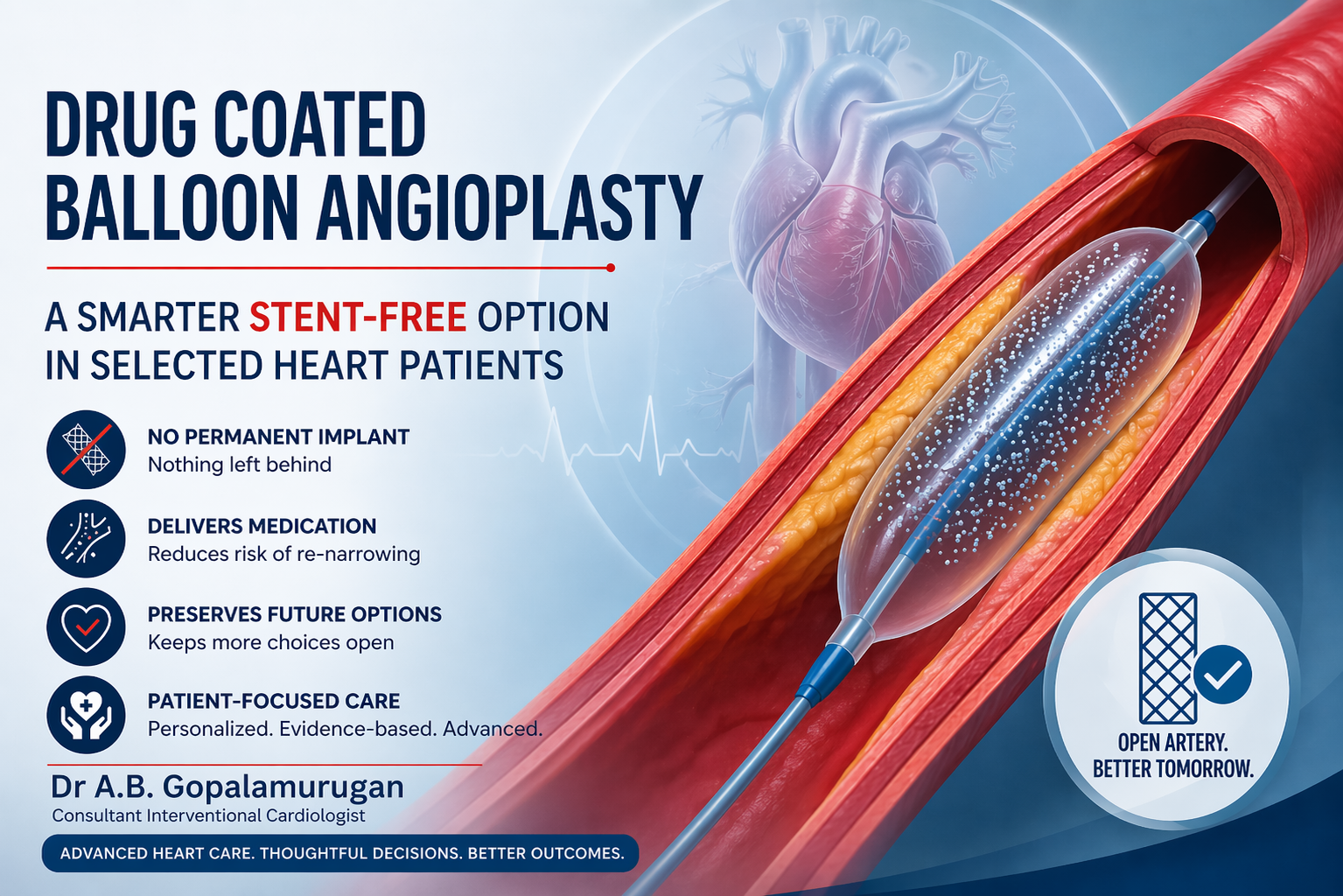
Drug Coated Balloon Angioplasty: A Smarter Stent-Free Option in Selected Heart Patients? | Dr. A B Gopalamurugan
When most people hear the word angioplasty, they immediately think of a stent. That is understandable, because stents have become one of the most common and effective ways to treat narrowed coronary arteries. But modern interventional cardiology is evolving, and in selected patients, treatment may sometimes be possible without leaving a permanent metal implant behind.
That is where drug coated balloon angioplasty comes in.
Also called DCB angioplasty or drug eluting balloon PCI, this approach uses a special balloon that not only opens the blocked artery, but also delivers medication directly to the vessel wall to reduce the chance of the artery narrowing again. The key difference is simple: after the balloon is removed, nothing permanent is left inside the artery. This “leave nothing behind” strategy is one of the main reasons drug-coated balloons have attracted so much attention in contemporary coronary intervention.
For patients exploring DCB angioplasty India, or trying to understand whether a drug-coated balloon could be an alternative to conventional stenting, the most important point is this: it is not a replacement for every stent procedure. It is a highly specialized option used in carefully selected situations, after detailed assessment of the artery, the blockage pattern, and the patient’s overall risk profile.
What Is Drug Coated Balloon Angioplasty?
A drug-coated balloon is an angioplasty balloon that carries an antiproliferative drug on its surface. When the balloon is inflated inside the narrowed artery for a short period, the drug is transferred to the vessel wall. The purpose of that drug is to reduce the abnormal healing response that can lead to re-narrowing, also called restenosis. Unlike a stent, the balloon is then removed, so there is no permanent scaffold left in the vessel.
In simple terms, standard balloon angioplasty opens the artery mechanically. A drug coated balloon does two things at once. First, it opens the narrowed area. Second, it delivers medicine locally to help keep the artery open afterward.
This is why many patients search online for terms such as balloon angioplasty without stent, drug eluting balloon PCI, or stent-free angioplasty.
How Is DCB Angioplasty Different from Stent Angioplasty?
In routine stent-based angioplasty, a metal scaffold called a drug-eluting stent is placed inside the artery to hold it open long term. That approach remains the standard treatment for many coronary blockages because it provides excellent immediate vessel support and strong long-term outcomes in a wide range of lesions.
Drug-coated balloon angioplasty is different because it avoids a permanent implant. That offers several potential advantages in the right patient. It avoids adding extra metal inside the artery, helps preserve natural vessel movement, may prevent multiple stent layers in previously treated segments, and can keep future treatment options more open if another intervention is needed later.
But that does not mean DCB is automatically better. A balloon-only strategy demands excellent lesion preparation, careful sizing, good final blood flow, and the absence of major vessel recoil or flow-limiting dissection. If those conditions are not met, a stent may still be the safer and more durable option.
When Is Drug Coated Balloon Angioplasty Most Useful?
The strongest and most established role of coronary DCB therapy is in in-stent restenosis. This happens when a previously treated artery becomes narrowed again inside an existing stent because of tissue growth or recurrent disease. In such cases, placing yet another stent can create multiple metal layers, which may not always be ideal. A drug-coated balloon offers a way to treat the restenosis without adding another stent layer.
Beyond in-stent restenosis, DCBs are also being used in selected cases of small vessel disease, certain bifurcation lesions, some diffuse lesions, and situations where avoiding a permanent implant may be beneficial. However, the evidence is not identical across all these scenarios. The role of DCBs outside restenosis is growing, but it remains case-dependent, and cardiologists must choose carefully.
That balance is important for patients to understand. Drug-coated balloons are exciting, but they are not a shortcut and not a universal substitute for stents.
Who May Be a Good Candidate for DCB Angioplasty?
A patient may be considered for drug coated balloon angioplasty when the cardiologist believes the blockage can be treated effectively without needing permanent scaffolding. That judgment depends on several factors.
These include whether the lesion is a previously stented segment with restenosis, whether the artery is small, whether the plaque can be prepared well before balloon delivery, whether the final angiographic result is stable after dilation, whether there is significant recoil or dissection after lesion preparation, and whether the overall anatomy favors a leave-nothing-behind approach.
In real practice, this decision is rarely based on one angiogram image alone. It often involves detailed procedural assessment and, in many advanced cath labs, support from intravascular imaging and expert lesion preparation techniques.
How Is the Procedure Performed?
From the patient’s perspective, DCB angioplasty feels broadly similar to a routine angioplasty procedure. The artery is accessed through the wrist or groin, a catheter is guided to the heart, and the narrowed coronary segment is crossed with a wire. The difference lies in what happens next.
Before a drug-coated balloon is used, the lesion usually needs careful preparation. This may include balloon dilatation with one or more devices to optimize the artery first. Only after the cardiologist is satisfied with the vessel preparation is the drug-coated balloon delivered and inflated for the required time to transfer the drug to the artery wall. The balloon is then removed.
If the result is excellent, no stent is implanted. If the result is not satisfactory, a stent may still be required as a bailout or definitive treatment.
This is why patients should think of DCB angioplasty not as “a simpler shortcut,” but as a precision technique that requires planning, experience, and sound judgment.
What Are the Potential Advantages of Drug Eluting Balloon PCI?
When used in the right setting, drug eluting balloon PCI offers some appealing clinical advantages.
1. No Permanent Implant
Nothing is left behind in the artery after treatment. This can be especially useful where another layer of metal would be undesirable.
2. Useful in In-Stent Restenosis
This remains one of the strongest indications. When a patient already has a stent and the same area becomes narrowed again, a drug-coated balloon may offer an effective way to treat that segment without placing another stent.
3. Potentially Preserves Future Options
Without an additional stent, future interventions may sometimes be easier to plan if needed later.
4. May Reduce Issues Related to Multiple Stent Layers
For patients who already have a stent in place, avoiding another implant can be a meaningful advantage.
5. A More Natural Vessel Strategy in Selected Cases
In certain situations, avoiding a permanent scaffold may help maintain a more natural vessel environment, especially when the lesion is well prepared and the final result is stable.
What Are the Limitations or Risks?
Patients should also know the limits of this technology.
A DCB does not provide the same mechanical scaffolding as a stent. If the artery recoils after balloon expansion, or if there is a major dissection, the result may not be durable or safe without a stent. That is why lesion preparation and final angiographic assessment are critical.
Another important point is that not all positive data apply equally to every lesion type. While DCB is well supported in restenosis and promising in other areas, stents still remain the preferred treatment for many untreated coronary blockages.
So, if a patient asks, “Can angioplasty be done without stent?” the honest answer is:
Yes, sometimes. But only in selected lesions and only when the artery can be treated safely and effectively without a permanent scaffold.
Drug Coated Balloon Angioplasty in India: Why Expertise Matters
As awareness grows around DCB angioplasty India, more patients are asking about stent-free options. That is a good thing, because informed patients often ask better questions. But the right question is not, “Can I avoid a stent at any cost?” The right question is, “What is the safest and most suitable treatment for my artery?”
A modern interventional cardiologist must decide between multiple strategies. These may include standard balloon angioplasty, drug-eluting stent implantation, drug-coated balloon angioplasty, atherectomy or advanced lesion preparation techniques, imaging-guided PCI, and hybrid approaches in complex disease.
The best treatment is the one that matches the artery, the plaque, the clinical situation, and the long-term interests of the patient.
Why This Topic Matters to Patients
Many people fear the idea of a permanent implant. Others have already had stents and are worried about repeat narrowing. Some want to know whether newer technologies can reduce the need for another layer of metal. Drug-coated balloon angioplasty addresses exactly these concerns.
It represents a more nuanced era in interventional cardiology, where treatment is no longer just about opening the artery, but about choosing the right device strategy for the right lesion. In selected patients, DCB can be elegant, effective, and highly valuable. But it works best when applied thoughtfully, not routinely.
Is DCB Angioplasty Suitable for Every Heart Blockage?
No. This is one of the most important things patients should understand.
Not every narrowed artery is suitable for a drug-coated balloon. Some blockages are heavily calcified. Some lesions are long, complex, or located in areas where vessel support is essential. In other situations, the artery may not respond well to balloon preparation alone. In such cases, stenting or another specialized intervention may provide a more predictable and durable result.
That is why treatment decisions should always be individualized. A procedure that is excellent for one patient may not be the best choice for another.
The Importance of Lesion Preparation
One of the most important concepts in drug coated balloon angioplasty is lesion preparation. Unlike stenting, where the scaffold helps hold the artery open after the procedure, DCB relies on the artery being well prepared beforehand.
This means the blockage must be opened properly, blood flow must be good, and the vessel should not show significant recoil or dangerous dissection. The final result has to be stable enough that a permanent implant is not necessary.
In many ways, this makes DCB a technique that demands both skill and discipline. The operator must know when the vessel is ready for balloon drug delivery and when the artery still needs stent support.
What Should Patients Ask Their Cardiologist?
Patients considering drug eluting balloon PCI or searching for DCB angioplasty India should not focus only on the hope of avoiding a stent. Instead, they should ask more meaningful questions:
Is my blockage suitable for a drug-coated balloon?
Is this being considered because of in-stent restenosis or a new blockage?
What happens if the artery does not respond well to balloon treatment alone?
Will I still need a stent during the procedure if the result is not adequate?
How will this choice affect long-term outcomes, medicines, and follow-up?
These questions often lead to a better and more realistic discussion about the procedure.
FAQs
1. What is drug coated balloon angioplasty?
Drug coated balloon angioplasty is a coronary intervention in which a special balloon opens the narrowed artery and delivers medication to the vessel wall to reduce re-narrowing. Unlike a stent, nothing permanent is left behind.
2. Is drug coated balloon angioplasty the same as stent angioplasty?
No. In stent angioplasty, a metal scaffold remains inside the artery. In DCB angioplasty, the balloon is removed after delivering the drug, so there is no permanent implant.
3. Can angioplasty be done without stent?
Yes, in selected cases. Balloon-only or DCB-based treatment may be possible when the lesion is suitable and the final result is stable without the need for scaffolding. However, many patients still benefit more from a stent.
4. When is a drug-coated balloon most commonly used?
One of the strongest and most established uses is coronary in-stent restenosis, where the artery narrows again inside a previously placed stent.
5. Is DCB angioplasty better than a stent?
Not universally. It can be an excellent option in the right lesion, but stents remain the preferred strategy in many coronary blockages. The choice depends on anatomy, lesion type, and procedural findings.
6. Is drug eluting balloon PCI available in India?
DCB technology is part of modern interventional cardiology practice and is discussed increasingly in advanced coronary care. Availability, indications, and suitability depend on the treating center and the cardiologist’s evaluation.
7. Does a drug-coated balloon reduce the chance of repeat blockage?
That is the intended purpose. The drug helps reduce restenosis by limiting abnormal tissue growth in the treated vessel segment.
8. Will I still need medicines after DCB angioplasty?
Yes, most patients will still need antiplatelet and other cardiac medicines after the procedure. The exact regimen depends on your clinical condition, artery findings, and your cardiologist’s recommendation.
About Dr A.B. Gopalamurugan
Dr A.B. Gopalamurugan is a Senior Interventional Cardiologist and Electrophysiologist with over 20 years of experience in advanced heart care. He is known for his expertise in Interventional Cardiology, TAVR, Electrophysiology, and Endovascular Aortic Repairs.
With a patient-focused and evidence-based approach, Dr Gopalamurugan is committed to offering advanced, thoughtful, and individualized treatment for a wide range of heart conditions, including coronary artery disease, complex angioplasty, heart rhythm disorders, and structural heart disease.
Qualifications
MD, MRCP, FRCP, CCDS, FACC
Consultation Locations
London
W1 Healthcare, 7 Russell Gardens,
London W14 8EZ, United Kingdom
Phone: +44 7425 861747
Chennai
2nd Floor, 46 & 48, Masilamani Rd, Balaji Nagar, Royapettah,
Chennai, Tamil Nadu 600014
Phone: 080560 88898
Mumbai
81-84, Indian Cancer Society Formerly Lady Ratan Tata Medical & Research Centre,
M.K. Karve Road, Cooperage St,
Mumbai, Maharashtra 400021
Phone: 089400 88898



