
 1 May, 2026
1 May, 2026
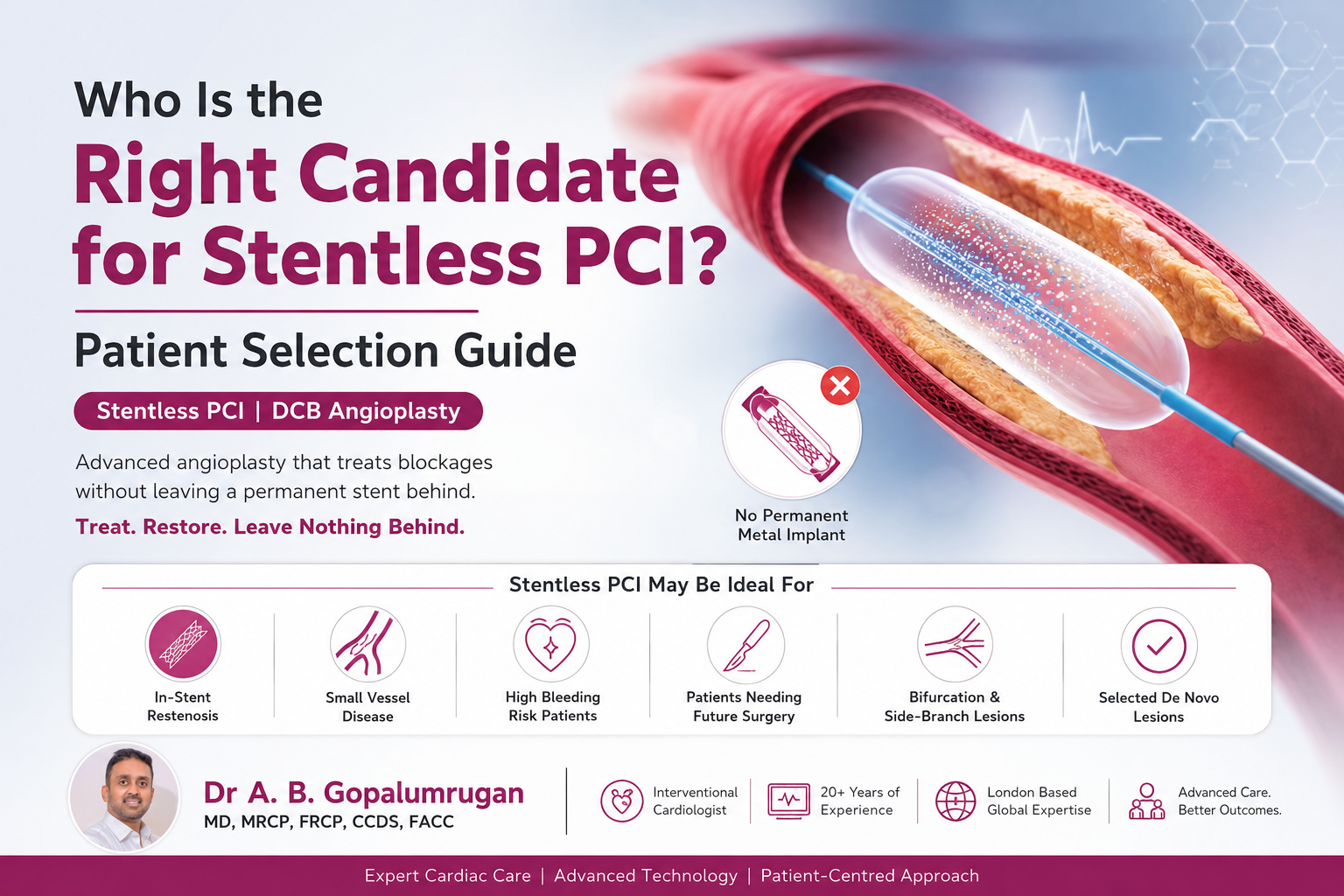
Who Is the Right Candidate for Stentless PCI? Patient Selection Guide
For many years, coronary angioplasty has been closely associated with stent placement. When a heart artery becomes narrowed or blocked, doctors often open the artery using balloon angioplasty and place a metallic stent to keep the vessel open. Stents have saved millions of lives and remain an important part of modern interventional cardiology.
However, not every patient needs a permanent metal implant inside the artery.
This is where Stentless PCI, also known as Drug-Coated Balloon angioplasty or DCB angioplasty, is becoming an important option for selected patients. Instead of leaving behind a metal stent, a drug-coated balloon delivers medicine directly to the artery wall and is then removed. The goal is to restore blood flow while leaving nothing permanent behind.
This approach is often described as a “leave nothing behind” angioplasty technique.
But the most important question is:
Who is the right candidate for Stentless PCI?
The answer depends on the type of blockage, the size of the artery, the quality of lesion preparation, previous stent history, bleeding risk, diabetes status, heart condition, and overall patient profile. Stentless PCI can be highly effective in the right patient, but it is not suitable for every coronary blockage.
What Is Stentless PCI?
Stentless PCI is a form of coronary angioplasty where a blocked or narrowed heart artery is treated without placing a permanent metallic stent.
In a conventional PCI procedure, the cardiologist opens the blocked artery using a balloon and then places a stent to support the vessel. In Stentless PCI, the artery is carefully prepared first. After that, a Drug-Coated Balloon is inflated inside the artery for a short period. During inflation, the balloon transfers anti-restenotic medicine to the artery wall. The balloon is then removed, and no metal scaffold is left behind.
This means the artery receives treatment without a permanent implant.
The success of Stentless PCI depends on proper case selection and excellent lesion preparation. If the artery opens well, blood flow is restored, and there is no major vessel recoil or dissection, the patient may be suitable for a stentless approach.
Why Patient Selection Is Important in Stentless PCI
Stentless PCI is not a one-size-fits-all treatment. It is a specialised technique that works best when the patient and the artery blockage are carefully selected.
The artery must be adequately opened before the drug-coated balloon is used. If the vessel has severe calcium, heavy recoil, long dissection, poor blood flow, or an unstable result after balloon preparation, a stent may still be required.
That is why the decision is usually made after a detailed angiogram assessment and, in many cases, with the support of advanced imaging such as OCT or IVUS.
Patient selection for Stentless PCI involves assessing:
- The location of the blockage
- The size of the artery
- The length of the lesion
- Whether the patient has a previous stent
- Whether the blockage is inside a stent
- The amount of calcium in the artery
- The result after vessel preparation
- The patient’s bleeding risk
- The need for long-term blood thinners
- Diabetes and kidney disease status
- Overall heart function
In experienced hands, this careful selection process helps identify patients who may benefit from a stentless angioplasty strategy.
Who May Be a Good Candidate for Stentless PCI?
1. Patients with In-Stent Restenosis
One of the most important indications for Drug-Coated Balloon angioplasty is in-stent restenosis.
In-stent restenosis means that a previously placed stent has narrowed again. This can happen because of tissue growth inside the stent or disease progression in the treated segment.
In such cases, placing another stent inside the old stent may create multiple layers of metal. This can make the artery less flexible and may complicate future treatment.
A Drug-Coated Balloon can treat the narrowed area by delivering medicine without adding another metal layer. This makes Stentless PCI especially useful for patients who already have a stent and are experiencing re-narrowing.
For many patients with in-stent restenosis, DCB angioplasty may help avoid the problem of “stent within stent.”
2. Patients with Small Vessel Coronary Artery Disease
Small vessel disease is common in India, especially among patients with diabetes, hypertension, and diffuse coronary artery disease.
In small arteries, even a small amount of tissue growth inside a stent can significantly reduce blood flow. Because the artery is already narrow, placing a metal stent may not always be the ideal long-term solution.
For selected small vessel blockages, Stentless PCI with a Drug-Coated Balloon may be considered. The balloon delivers medicine to the artery wall and is removed, avoiding a permanent metallic implant in a small vessel.
This may be especially useful when the artery is too small for comfortable stent placement or when the cardiologist wants to preserve the natural structure of the vessel.
3. Patients Where Avoiding Extra Metal Is Important
Some patients already have multiple stents. Others may have long segments of disease where placing more metal may not be ideal.
Stentless PCI may be considered when the doctor wants to avoid:
- Multiple stent layers
- Very long stented segments
- Metal across side branches
- Unnecessary permanent implants
- Complex future re-intervention
This is particularly relevant in younger patients, patients with repeat coronary procedures, and patients with complex coronary anatomy.
The “leave nothing behind” concept is important because once a stent is placed, it becomes a permanent part of the artery. In selected patients, avoiding unnecessary metal may help preserve future treatment options.
4. Patients with Bifurcation or Side-Branch Lesions
A bifurcation lesion occurs where one artery divides into two branches.
Stenting in bifurcation areas can sometimes be complex because the stent may cover or affect a side branch. In selected cases, Drug-Coated Balloon angioplasty may be useful to treat the side branch or avoid unnecessary stenting across important branch points.
This does not mean every bifurcation blockage is suitable for Stentless PCI. Some complex bifurcation lesions may still require stenting. However, when the anatomy is favourable and the artery responds well to preparation, a DCB-based strategy may help reduce the amount of metal used.
5. Patients with High Bleeding Risk
After stent placement, patients usually need dual antiplatelet therapy for a certain duration. These medicines are important to prevent clot formation inside the stent.
However, some patients have a higher risk of bleeding. This may include elderly patients, patients with previous bleeding episodes, patients needing surgery soon, or those with other medical conditions requiring blood thinners.
In selected high-bleeding-risk patients, Stentless PCI may be considered because there is no permanent metal implant left behind. The duration and type of blood-thinning treatment must always be decided by the treating cardiologist based on the individual patient’s condition.
This can be an important consideration for Indian patients who may have multiple health conditions, upcoming surgeries, or difficulty tolerating prolonged blood thinners.
6. Patients Who May Need Future Surgery
Some heart patients may need non-cardiac surgery in the near future, such as cancer surgery, orthopaedic surgery, abdominal surgery, or urological procedures.
When a stent is placed, surgery may need to be delayed depending on the patient’s antiplatelet therapy requirements and overall cardiac risk. In carefully selected patients, Stentless PCI may offer flexibility by avoiding a permanent implant.
However, this decision must be made very carefully. The cardiologist will assess the urgency of surgery, the severity of the heart blockage, the risk of delaying surgery, and the safest revascularisation plan.
7. Patients with Diabetes and Diffuse Coronary Disease
India has a high burden of diabetes, and diabetic patients often develop diffuse coronary artery disease. Their arteries may have long, narrow, and multiple blockages rather than one simple focal narrowing.
In some diabetic patients, stenting remains necessary and beneficial. In others, especially where small vessels or restenosis are involved, a Drug-Coated Balloon strategy may be considered.
The key factor is not diabetes alone, but the pattern of coronary disease. If the blockage is suitable, the vessel can be well prepared, and the angiographic result is good, Stentless PCI may be an option.
For diabetic patients, careful imaging, vessel sizing, and lesion preparation are especially important.
8. Patients with De Novo Coronary Lesions
A de novo lesion means a new blockage in an artery that has not been previously stented.
Traditionally, DCB angioplasty was more commonly used for in-stent restenosis and small vessel disease. Today, with better devices, improved techniques, and advanced imaging, selected de novo lesions may also be treated with a stentless strategy.
However, this requires careful judgment. The lesion should be suitable for balloon preparation, the artery should maintain good flow, and there should not be significant recoil or major dissection after preparation.
A stentless approach for de novo lesions should be performed by experienced operators who understand when DCB is appropriate and when a stent is safer.
When Is Stentless PCI Not Suitable?
Stentless PCI is not suitable for every patient. In some cases, placing a stent may still be the better and safer option.
Stentless PCI may not be ideal in cases of:
- Large vessel blockage requiring strong mechanical support
- Severe vessel recoil after balloon angioplasty
- Major dissection after lesion preparation
- Heavy calcification that cannot be adequately modified
- Long complex blockages where the artery does not open well
- Poor blood flow after balloon preparation
- Acute unstable situations where stenting is clearly required
- Left main or highly complex lesions where a stent strategy is more appropriate
The final decision depends on the angiogram, the patient’s clinical condition, and the cardiologist’s assessment during the procedure.
Role of Lesion Preparation in Stentless PCI
Lesion preparation is one of the most important steps in Stentless PCI.
Before using the Drug-Coated Balloon, the artery must be properly opened. This may involve:
- Pre-dilatation with a balloon
- Scoring balloon
- Cutting balloon
- High-pressure balloon
- Calcium modification techniques
- Intravascular imaging guidance
The purpose is to create a smooth and adequate opening in the artery so that the drug-coated balloon can deliver medicine effectively.
If the vessel preparation is poor, the result may not be durable. If the artery is well prepared and the final result is stable, Stentless PCI may be successful.
This is why Stentless PCI is not just about using a DCB. It is about using the right technique, in the right vessel, for the right patient.
Role of OCT and IVUS in Patient Selection
Advanced imaging tools such as OCT and IVUS can help cardiologists see the artery from inside.
These technologies may help assess:
- Vessel size
- Plaque type
- Calcium burden
- Stent expansion in previous stents
- Cause of in-stent restenosis
- Whether the lesion is properly prepared
- Whether a stent is needed
- Final result after angioplasty
For Stentless PCI, imaging can be extremely helpful because the doctor needs to confirm that the artery has opened properly and that the result is stable.
In complex cases, OCT or IVUS-guided PCI may improve decision-making and procedural precision.
Benefits of Stentless PCI in Selected Patients
When used in the right candidate, Stentless PCI may offer several potential advantages.
1. No Permanent Metal Implant
The biggest advantage is that no metal stent is left behind. This preserves the natural structure of the artery.
2. Useful for In-Stent Restenosis
It can treat re-narrowing inside a previous stent without adding another stent layer.
3. Helpful in Small Vessels
It may be beneficial in selected small-vessel blockages where placing a stent may be less ideal.
4. Preserves Future Treatment Options
Because no new metal is placed, future procedures may be easier if needed.
5. May Reduce Long-Term Implant-Related Concerns
Some long-term issues related to permanent metal implants may be avoided in suitable patients.
6. Supports the “Leave Nothing Behind” Approach
This modern concept focuses on treating the disease while avoiding unnecessary permanent material inside the artery.
Stentless PCI in India
India has a growing number of patients with coronary artery disease. Diabetes, hypertension, high cholesterol, smoking, sedentary lifestyle, stress, and family history are common risk factors.
Many Indian patients also present with complex coronary disease, small vessels, diffuse blockages, and repeat narrowing after previous angioplasty.
In this context, Stentless PCI is becoming an important treatment consideration in selected cases. It is especially relevant for patients with:
- Small vessel coronary disease
- In-stent restenosis
- Diabetes-related diffuse disease
- Previous multiple stents
- High bleeding risk
- Complex anatomy where avoiding extra metal is beneficial
However, it is important to understand that Stentless PCI should be performed only after careful evaluation. The treatment should be individualised, and the decision must be made by a skilled interventional cardiologist.
Questions Patients Should Ask Their Cardiologist
If you are being evaluated for angioplasty, you can ask your cardiologist:
- Am I suitable for Stentless PCI?
- Is my blockage in a small vessel or large vessel?
- Do I have in-stent restenosis?
- Can my artery be treated with a Drug-Coated Balloon?
- Will I need a stent, or can it be avoided?
- Is OCT or IVUS needed in my case?
- What are the benefits and risks of DCB angioplasty for me?
- How long will I need blood thinners after the procedure?
- What happens if the artery does not open properly during the procedure?
These questions can help patients understand their treatment options clearly.
Stentless PCI is an advanced angioplasty technique that allows selected coronary artery blockages to be treated without leaving behind a permanent metal stent. It is especially useful in carefully chosen patients with in-stent restenosis, small vessel disease, certain bifurcation lesions, high bleeding risk, or cases where avoiding additional metal is important.
However, the success of Stentless PCI depends on correct patient selection, proper lesion preparation, advanced imaging when required, and the experience of the treating cardiologist.
Not every patient is a candidate for Stentless PCI. Some blockages still require stenting for the best and safest result. The right approach should always be personalised based on the patient’s artery anatomy, medical condition, and long-term treatment needs.
For patients in India, the key message is simple: Stentless PCI can be an excellent option for the right candidate, but the decision must be made after expert cardiac evaluation.
About Dr A. B. Gopalamurugan
Dr A. B. Gopalamurugan is a London-based cardiologist with over 20 years of experience. He is widely known for his work in interventional cardiology, TAVR, electrophysiology, and endovascular aortic repairs.
He has trained and worked internationally and has extensive experience in complex cardiac interventions, including advanced coronary procedures, structural heart interventions, and electrophysiology treatments.
For Indian patients seeking advanced heart care, expert evaluation is essential before choosing between conventional stent angioplasty and Stentless PCI.
FAQs
1. What is Stentless PCI?
Stentless PCI is an angioplasty technique where a blocked heart artery is treated without placing a permanent metal stent. A Drug-Coated Balloon is used to deliver medicine to the artery wall and is then removed.
2. Who is the right candidate for Stentless PCI?
Patients with in-stent restenosis, small vessel disease, selected de novo lesions, high bleeding risk, or those where avoiding extra metal is important may be considered for Stentless PCI.
3. Is Stentless PCI better than stent angioplasty?
Stentless PCI is not always better than stenting. It is better only for selected patients and specific types of blockages. Some patients still need a stent for the safest and most durable result.
4. What is DCB angioplasty?
DCB angioplasty, or Drug-Coated Balloon angioplasty, uses a special balloon coated with medicine. The medicine is delivered to the artery wall to reduce the chance of re-narrowing.
5. Is Stentless PCI suitable for diabetic patients?
Some diabetic patients may be suitable, especially if they have small vessel disease, diffuse disease, or in-stent restenosis. However, the decision depends on the angiogram and cardiologist’s assessment.
6. Can Stentless PCI treat a previously placed stent that has narrowed again?
Yes. In-stent restenosis is one of the most common situations where Drug-Coated Balloon angioplasty may be considered.
7. Does Stentless PCI mean no blood thinners are needed?
No. Blood-thinning medicines may still be required after the procedure. The type and duration depend on the patient’s condition and the cardiologist’s recommendation.
8. Is Stentless PCI available in India?
Yes, Stentless PCI and DCB angioplasty are available in selected advanced cardiac centres in India. It should be performed by experienced interventional cardiologists after proper evaluation.
9. Can every blockage be treated without a stent?
No. Some blockages require a stent, especially if there is severe recoil, major dissection, poor blood flow, or complex anatomy.
10. How do doctors decide between stent and Stentless PCI?
Doctors assess the angiogram, artery size, blockage type, calcium burden, lesion preparation result, imaging findings, and patient risk factors before deciding.
Stentless PCI India | Stentless angioplasty India | Drug-Coated Balloon angioplasty India | DCB angioplasty India | who qualifies for stentless angioplasty | stentless PCI patient selection | DCB angioplasty candidate | coronary angioplasty without stent | angioplasty without stent India | leave nothing behind angioplasty | drug coated balloon PCI | DCB PCI India | in-stent restenosis treatment India | small vessel coronary artery disease treatment | small vessel angioplasty India | stentless heart procedure | advanced coronary angioplasty India | best cardiologist for stentless PCI India | Dr A B Gopalamurugan cardiologist | Dr AB Gopalamurugan Stentless PCI | interventional cardiologist India | complex coronary angioplasty India | OCT guided PCI India | IVUS guided PCI India | DCB for in-stent restenosis | DCB for small vessel disease | stentless PCI for diabetic patients | heart blockage treatment without stent | advanced angioplasty treatment India



